Achilles Tendon Rupture

What is it?
A tear of the Achilles tendon refers to a tear within the large tendon which joins the calf muscles (gastrocnemius and soleus) to the heel bone (calcaneus). See figure 1 (a) and (b) which provides an illustration of what actually has happened.
How did I get it?
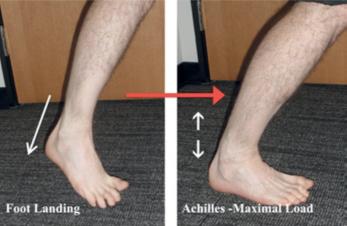
Tears of the Achilles tendon occur when the calf muscles are forcibly contracted. The function of the Achilles tendon is to transmit forces produced by the calf muscles to the heel bone. Forcible contraction of these muscles can overstress the Achilles tendon, resulting in a complete tear. This can occur during lunging for a ball in racquet sports or jumping in sports such as volleyball and basketball. See figure 2 which illustrates some of the more common lower leg positions which can produce sufficient force/s on the achilles that over time will deteriorate this tendon. Usually the activity resulting in tendon tear has successfully been performed many times in the past. Often the tendon has suffered wear and tear and has degenerated prior to the injury.
What are the symptoms?
A complete tear of the Achilles tendon results in immediate agonising pain at the back of the heel. This pain is often described as a sensation of being hit or kicked in the back of the leg. Associated with this may be a feeling of something tearing or snapping. Following a complete tear of the Achilles tendon it is extremely unlikely you will be able to continue participating in the activity or sport. There will be substantial weakness in the calf and this will impact your ability to walk normally due to both the pain and weakness.
A partial tear can be more subtle. Often there will be a sharp sudden pain in behind the heel although sometimes the pain may have an insidious onset.
What should I do?
A tear of the Achilles tendon is a potentially serious injury which requires urgent review. A complete tear of the Achilles tendon is a serious injury which does not heal by itself without appropriate treatment. If you have or suspect you have a tear of the Achilles tendon it is advisable you seek the assistance of a sports medicine professional as soon as possible. In the interim you can commence early treatment to limit the amount of internal bleeding and swelling within and around the tendon. Bleeding, swelling and inflammation are outcomes with any Achilles tear. It is useful in the early stages to try to decrease the amount of swelling. Early management should involve RICE treatment. (Rest, Ice, Compression and Elevation)
There are many injuries that you can train through or around but this is not one of them. Continuing to attempt to play with a torn Achilles could result in a long term disability. Rest involves ceasing activity and limiting the amount of weight you put through your leg. Crutches can be used if there is difficulty walking.
Ice is very useful initially and helps decrease the amount of swelling. Usually 10 mins on, 10 mins off, 10 mins on, every 2 hours is effective and decreases the likelihood of nerve damage from ice burn.
Compression and elevation will assist to decrease the amount of swelling.
How is a diagnosis made?
Diagnosis is usually made with history and examination. Sometimes extra scans such as x-ray, ultrasound or MRI are required if the symptoms and examination findings are not typical.

What does rehab involve?
A decision regarding treatment needs to be determined as soon as possible after the injury occurs. This will ensure further damage is limited or contained.
Partial Tears
Partial Achilles tears can usually be managed without surgery. The pain, swelling and inflammation need to be managed cautiously in the initially stages and this is done under the guidance of your sport’s medicine professional. A large or severe tear may require a cast or walking boot. After the initial pain and swelling has subsided partial tears can usually be treated as a severe case of Achilles tendinopathy and undergo a functional rehab and strengthening program.
Complete Rupture
There is some controversy regarding which patients are better suited to surgical vs non-surgical management of complete Achilles tendon ruptures. Most of the studies show that there is little difference between overall satisfaction or return to activity, between surgical and non-surgical management. There is however, a higher re-rupture rate in the non-surgery group. Studies have shown the re-injury rate without surgery is more than double that with surgery. The two main studies have shown re-injury rates of 12% and 8% for that group not having surgery while the re injury rates in those having the surgery were lower at 5% and 3%. The risk though of other complications (such as skin infection) is higher in the surgical group. Given that the activity and quality of life measures are the same with and without surgery the decision essentially becomes one of weighing up the risks of re-rupture vs the risk of operative complications and infections.
Intuitively it would seem that the young active group who are likely to engage in high risk activities / sports and who would have a low risk for complications might choose the surgery option while the decision is less clear for other groups.
Non-surgical Management
In a patient who has the required strength to operate crutches, the preferred management of this injury would require the patient to have a cast on the ankle in plantar flexion (toes pointing down, like a ballet dancer en pointe). The image above illustrates this position that the plastered foot would be in. Over a period of months the cast will be removed and reapplied with the ankle in slightly less of a pointed position each time until the foot is at 90 degrees with the shin. In an older patient with multiple other medical problems and / or who does not have the ability to operate on crutches a walking boot may be the only alternative. This should still result in repair however it is not considered to be as effective as the previous management option i.e. cast and crutches.
Surgical Management
Surgery usually needs to be performed within a couple of weeks of the injury or it becomes very difficult due to scar tissue formation. The leg is usually put in a cast with the ankle in plantar flexion – toes pointing down, like a ballet dancer en pointe (see image below). Depending on the rehab protocol there may be early or delayed weight bearing in a walking boot.